

Sonita Kamara is in obstructed labour, a life-threatening complication where the baby cannot pass through the birth canal despite strong contractions. She is rushed to Princess Christian Maternity Hospital (PCMH) in Freetown, the busiest maternity and newborn hospital in Sierra Leone.
Her baby is in distress. “If we don’t operate within 30 minutes, the baby might die,” says Dr Rosetta Cole, senior obstetrician-gynaecologist, as she prepares to perform an emergency caesarean section.
But the operation cannot begin. The hospital has run out of basic surgical supplies: sutures, anaesthetic and IV fluids. Kamara’s family is sent into the city to search for them in pharmacies. More than two hours later, they return and the operation can finally start.
After an agonising wait, Kamara’s newborn is safely delivered but is in need of oxygen. Baby Kelvin is transferred a few metres away to the special care baby unit at Ola During Children’s Hospital. A few days later, he and Kamara are discharged.
Not every mother in Sierra Leone is so lucky.
In collaboration with documentary team, On Our Radar, Fuller spent a week following the people working in Sierra Leone’s leading maternity hospital. The resulting film tells the story of their passion and commitment, the progress Sierra Leone has made in reducing maternal mortality and how, following drastic aid cuts by the UK and US, that progress now hangs in the balance.
The funding shock and the fall out
A small nation of close to nine million people on the west coast of Africa, Sierra Leone is one of the world’s poorest countries and depends heavily on foreign aid to fund essential services, including in healthcare. In 2023, it received close to $500m in official development assistance and total aid flows have, at times, exceeded 10% of the country’s total economic output.
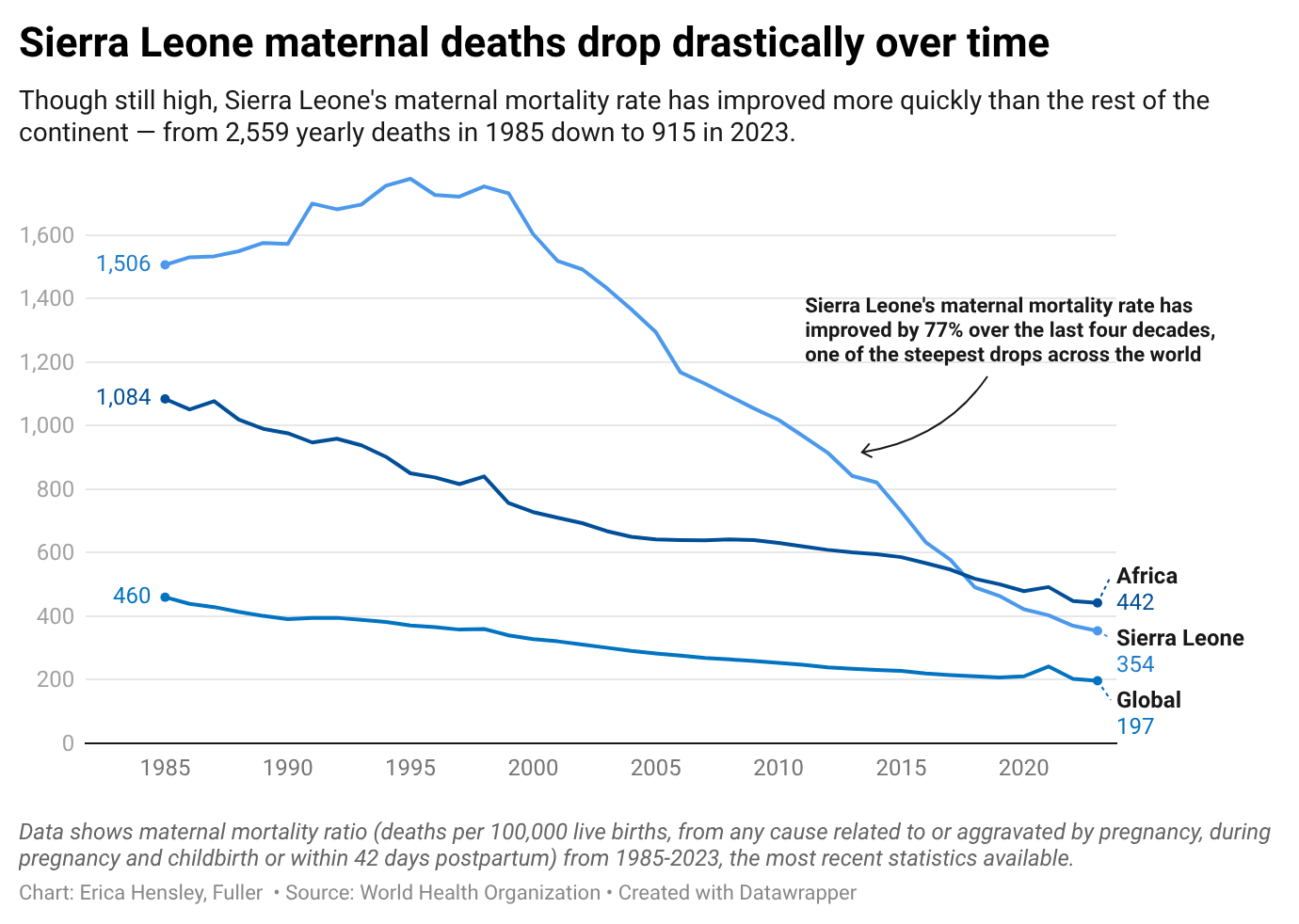
Sierra Leone once had the third-highest maternal mortality rate in the world but, since 2000, maternal deaths have fallen by nearly 80%. Foreign aid has been credited with helping more Sierra Leonean women and children survive childbirth.
The special care baby unit at Ola During Children’s Hospital, to which Sonita Kamara’s baby was sent, was built – and gets money for supplies – through the Saving Lives in Sierra Leone programme.
Started in 2016 with funding entirely provided by the UK, the work of Saving Lives (which has included training for midwives, the provision of contraceptives and the establishment of special care baby units) had previously been a source of pride for British politicians. In 2023, it was renewed for a third, five-year phase and allocated a budget of £35 million ($47.3 million).
Then, without warning, the entire system was thrown into turmoil. At the end of January 2025, the Trump administration issued a stop-work order, abruptly freezing projects funded by USAid around the world. In February, British prime minister Keir Starmer delivered a further shock: UK aid would be cut from 0.5% to 0.3% of gross national income. Then, in March, confirmation came that 83% of USAid programs would be cancelled.
Despite Starmer saying funding would fall from 2027, by late 2025 it was reported that Saving Lives had been axed “quietly behind the scenes”; its remaining funding of approximately £17 million ($22.9 million) reduced to just £1 million ($1.3 million). Sources close to the programme confirmed this, telling Fuller that they thought activities could be wound down as soon as March 2026.
A Foreign Office spokesperson would neither confirm nor deny the cuts, telling Fuller: “Allocations of the official development assistance budget for next year haven’t been set out yet and we will not speculate on them in advance.”
The impact of the loss of US funding has been harder to show clearly because “when US funding is cut, it affects our health institutions … not only in maternal and child health but also in other critical areas,” explains Dr Mustafa Kaba, deputy chief medical officer for clinical services at the Ministry of Health and Sanitation in Sierra Leone.
The ministry told Human Rights Watch in July that cuts in US foreign aid represented a $45 million reduction in health projects focused on maternal, child, and adolescent health. And in 2024, the US provided $3.2 million to Sierra Leone’s reproductive health, about 14% of the country’s overall reproductive health funding.

Despite lively debate on the effectiveness and ethics of aid, the consensus has been that its abrupt termination was irresponsible, would disproportionately affect women and girls around the world and invariably lead to more deaths.
“The sudden nature of these cuts is a huge blow,” says Dr Nellie Bell, head of paediatrics at Ola During Children's Hospital. “We are already stretched … but we are going to see an increase in mortality in all those [special care baby] units.”
Claudia Craig, a senior advocacy adviser at Care International UK, who worked on previous phases of the Saving Lives programme, says the UK government had been warned what impact an abrupt termination of funding would have.
“Despite evidence and sustained warnings that these cuts would put women and girls at risk, we were ignored. Today, the consequences are unfolding in real time. The suffering is not inevitable. It is the foreseeable result of deliberate policy choices,” she says, before adding: “It is not too late to change course.”
"I am not a fan of aid dependency,” Freetown mayor, Yvonne Aki-Sawyerr, tells Fuller. “But when aid is removed in the context of weak governance, mismanagement and corruption, you increase the population’s vulnerability.”
A year on, can Sierra Leone maintain maternal health progress and keep women from dying needlessly in childbirth?
Aid as coercion
Asked where Sierra Leone was at in its negotiations and commitments with the US and UK, Dr Kaba says the Ministry of Health is still engaging with the UK Foreign Office and embassy, but have not yet received concrete answers.
As for the US, he pointed to a recently signed bilateral agreement. The memorandum of understanding is part of the America First Global Health Strategy (AFGHS) which sets out how Washington intends to engage in global health going forward. A press release from December, suggests that the US Department of State will “front-load” more than $30 million into the country's health systems in 2026, “while Sierra Leone steadily increases its own financial contributions”, as well as announcing hundreds of millions more in funding up until 2030.
The administration has said AFGHS is about “reducing foreign dependency on US taxpayers” and about “helping countries move toward more resilient and durable health systems” – but civil society groups disagree.
“AFGHS is being framed as health assistance, but it’s about corporate interests,” says Fadekemi Akinfaderin, chief global advocacy officer at feminist alliance Fòs Feminista. They published an analysis of the Global Health Strategy and concluded that it is “a vehicle for advancing US military and commercial interests through increasingly coercive tactics”.
With little transparency, it is unclear whether the sums announced are already being spent, what they are specifically being spent on, and what Sierra Leone has offered in return for continued US funding.

Creating a system that depends on itself
According to Dr Kaba, health funding into Sierra Leone has traditionally flowed predominantly through UN agencies such as WHO, Unicef and UNFPA, as well as international NGOs, making it hard for even the Ministry of Health to fully quantify the extent of the country's foreign aid dependency.
“It has been very difficult to estimate,” Dr Kaba says. “When US funding was cut, we tried to assess its impact on the health sector – not only on maternal health – but it was challenging to get accurate data and figures”.
There are other funding sources for maternal and child health efforts in Sierra Leone, including countries such as Japan, China, Sweden, Canada, Germany, Ireland and development banks. For instance, in 2021, the World Bank invested $60 million in a project to deliver maternal and child health and nutrition services. This runs through to 2027.
One way to compensate for lost funding would be to raise money for public services through taxation. But the latest revenue statistics from the OECD show that Sierra Leone’s tax revenue, relative to the size of its economy, is approximately 11% – below what the World Bank recommends for “inclusive growth and development” (15%) and less than the African average, 16%. The 2026 government budget, however, does propose a series of new taxes, intended to “yield 1.5% of GDP in additional revenues by 2027”.
Abou Bakarr Kamara, senior economist at Sierra Leone’s International Growth Centre, tells Fuller: “Implementation depends on the capacity of national revenue institutions and that can take years”.
Despite the challenges ahead, Dr Kaba at the health ministry isn’t fearing the worst. Instead, he sees the drastically changing aid landscape as an opportunity for Sierra Leone. “We are not assuming the health sector will collapse,” Dr Kaba says. “It is a moment to realign, adjust to realities and strengthen innovative health financing schemes. If support comes in the future, we welcome it. But we want a resilient system that depends on itself.”
At a meeting of the Africa Union in February, Sierra Leonean president, Julius Maada Bio, launched a 300-day campaign aimed at “ensuring continuous care throughout pregnancy, promoting safe deliveries, responding swiftly to complications, and providing thorough postnatal follow-up”. The campaign starts 1 March but at time of writing no specifics details, targets or projects had been made public.
For the mothers, doctors and nurses of Princess Christian Maternity Hospital and Ola During Children’s Hospital, the decisions of two men – the US president and British prime minister – are likely to have far-reaching consequences. It remains to be seen whether Sierra Leone's president can find other ways to ensure Sonita Kamara’s story of survival isn't once again the exception.
In the original version of this article, Claudia Craig was incorrectly anonymized. This has been corrected to reflect that they provided an attributable quote.
Edited by Eliza Anyangwe and Charlie Brinkhurst-Cuff. Data reporting by Erica Hensley. Visual editor Lara Antal. Lead visuals by Nathalie Basoski. Stills from Fuller video documentary, produced by On Our Radar.
Edited by Eliza Anyangwe and Charlie Brinkhurst-Cuff. Data reporting by Erica Hensley. Visual editor Lara Antal. Lead visuals by Nathalie Basoski. Stills from Fuller video documentary, produced by On Our Radar.